

By Jessica Duke, MD
With winter storms bringing cold, wind, and snow across much of the United States, let’s review some important points about hypothermia.
Accidental hypothermia is an unintentional drop in core temperature to 35°C/95°F or below. Hypothermia is classified as mild (35-32°C/95-90°F), moderate (32-28°C/90-82°F), severe (28-24°C/82-75°F), or profound (<24°C/75°F). It is very difficult to accurately measure core temperature in the wilderness so physical exam findings are used to assess cold-exposed patients.
Someone with mild hypothermia will be alert, but have impaired movement and uncontrolled shivering. Shivering increases metabolic heat production and helps prevent hypothermia as long as the patient has sufficient energy reserves to sustain shivering and is adequately insulated from the environment to retain the heat that is generated. Resting for 30 minutes, eating and drinking, passive rewarming (moving to a warm environment, removing wet clothing, and insulating in warm layers or a hypothermia wrap), and active external warming (drinking warm beverages and applying hot water bottles, large heating packs, or heating blankets to the core) should be sufficient to treat mild hypothermia. If re-warming is not possible or the victim does not improve with these interventions, they will need to be evacuated.
A person with moderate hypothermia will have an altered mental status and will eventually stop shivering as they use up their energy reserves. If they lose vasomotor tone, the hypothermic patient may feel overheated and want to take off their clothing/layers as warm blood from the core suddenly floods the extremities. This is a phenomenon known as paradoxical undressing. These patients need to be handled gently as their hearts are at high risk for arrhythmia. Rewarming methods should focus on warming the patient’s core with the patient in a horizontal position to avoid core afterdrop (when cold blood from the extremities returns to the core), as this can lead to further hemodynamic instability. In addition to passive rewarming and active external rewarming, active internal warming (warm IV fluids) should also be initiated, if available. These patients will need to be evacuated.
Victims of severe or profound hypothermia will be unconscious. These patients will have depressed cardiac activity and slow respirations so it is important to feel for a pulse and look for breathing for a full minute. If the patient shows signs of life, their breathing should be assisted and they should be rewarmed as in moderate hypothermia. If the patient does not have a pulse and has not sustained a lethal injury or prolonged asphyxiation, CPR and rewarming should be performed until the patient’s core temperature has reached 30°C/86°F (“nobody is dead until warm and dead”). Advanced life support drugs and defibrillation are typically ineffective below this temperature, but one shock can be delivered if indicated. If unsuccessful, AED use should be discontinued until the core temperature has reached 30°C/86°F. Ideally, these patients should be evacuated to a hospital with extracorporeal circulation capability.
For more details on these recommendations, check out the Wilderness Medical Society practice guidelines for the out-of-hospital evaluation and treatment of accidental hypothermia. Their recommendations are summarized in the flow chart below.

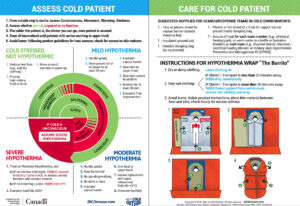
For a great reference guide, look over Dr. Gordon Giesbrecht’s “Cold Card” in the latest Wilderness & Environmental Medicine journal. This 2-sided card is a concise summary to aid responders in the assessment and field care of cold-exposed patients. See below for the card and consider carrying it (and the necessary supplies) with you on cold weather excursions.
References:
Giesbrect GG. “Cold Card” to Guide Responders in the Assessment and Care of Cold-Exposed Patients. Wilderness Environ Med. 2018;29(4):499-503.
Zafren K, Giesbrecht GG, Danzl DF, Brugger H, Sagalyn E, Walpoth B, et al. Wilderness Medical Society practice guidelines for the out-of-hospital evaluation and treatment of accidental hypothermia. 2014 update. Wilderness Environ Med. 2014;25(4 suppl):S66-85.